September 9, 2025-OrthoSpineNews-
Author: Javad Parvizi, MD, – Submitted by: The International Joint Center, a part of the Acıbadem Healthcare Group
Femoroacetabular impingement (FAI) is a condition that’s probably been around for as long as hip arthritis has been around. It is an abnormal anatomy of the hip. Either the femoral head and or the acetabulum are abnormal, leading to an abnormal mechanical contact between femoral neck and rim of the acetabulum, which then causes labral tear, and eventually wear of the articular cartilage in arthritis.
It is a condition that was described in the 1930s by Smith Peterson, from Boston, and was popularized by me and Professor Ganz in one of our first published papers on the subject. [1] Femoroacetabular impingement significantly impacts long-term hip preservation outcomes, with studies showing 12% of patients requiring conversion to total hip arthroplasty (THA) after a mean follow-up of 12.5 years. We often see varying results between different surgical approaches for this condition. For instance, patients with borderline dysplasia (BD) show notably better outcomes, with only 5.3% requiring revision surgery compared to 10.4% in control groups.
Research shows survivorship rates of 87% at 5 years and 79% at 10 years for patients avoiding conversion to THA. However, certain risk factors like older age, longer symptomatic periods, and full-thickness acetabular chondral lesions can increase failure rates. And, as we better understand this condition we are seeing more patients with FAI. And, if we catch it earlier before it’s arthritis, we can potentially do what we call joint preservation procedure. This requires removing the impingement, repairing the labrum, and patients do well in terms of their functional limitation and pain, but eventually it leads to arthritis. And these patients are young when they develop arthritis, and at that time, obviously THA is the right option for them.
In this article, we’ll examine the complex relationship between FAI and THA outcomes, exploring patient selection criteria, surgical techniques, and predictive factors that influence long-term success. Additionally, we’ll investigate how proper treatment approaches can potentially delay or prevent the need for more invasive procedures.
Understanding Femoroacetabular Impingement in the Context of THA
Abnormal hip joint morphology forms the basis of FAI, a condition that creates significant clinical implications for THA planning and outcomes. Understanding the underlying mechanics of this condition is essential for orthopedic surgeons considering intervention options.
The challenges of doing a THA in young patients is the durability of the prosthesis. Especially if they are young and active. These patients put a lot of cycles across the prosthetic hip and wear it out eventually. And extreme activity can also result in dislocation.
What is femoroacetabular impingement (FAI)?
FAI is a pathomechanical process that occurs when the proximal femur abnormally contacts the acetabular rim [1]. Rather than being a disease itself, FAI represents a mechanical condition where extra bone growth along one or both hip joint bones creates an irregular shape [1]. This irregular morphology prevents normal movement, causing friction that ultimately damages joint structures [1].
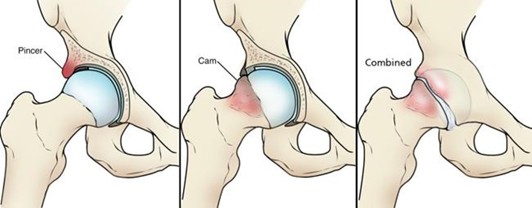
FAI manifests in three distinct forms:
- Cam impingement: Characterized by an aspherical femoral head or a bony prominence at the femoral head-neck junction, predominantly affecting young athletic males in their 20s or 30s [2]
- Pincer impingement: Features acetabular over coverage with an overly prominent rim, typically presenting in middle-aged women engaged in activities like yoga or aerobics [2]
- Combined impingement: Involves both cam and pincer morphologies simultaneously, representing up to 80% of cases [3]
(OrthoInfo: Femoroacetabular Impingement. Accessed 2025)
The prevalence of FAI in the general adult population ranges between 10-15%, though this increases dramatically to 55% among symptomatic athletes [2]. Furthermore, studies indicate cam deformity prevalence reaches 54.8% in athletes compared to just 23.1% in non-athletes [2].
Cam-type femoroacetabular impingement and acetabular coverage
Cam-type impingement occurs when the femoral head lacks sphericity or there is insufficient femoral head-neck offset [1]. This structural abnormality causes the non-spherical portion to abnormally pressurize the cartilage at the acetabular rim during hip flexion, initiating chondral and subsequent labral damage [1]. Essentially, the aspherical femoral head or bump at the femoral head-neck junction grinds against the cartilage inside the acetabulum [2].
The alpha angle measurement provides a key diagnostic indicator for cam deformity. Values exceeding 60 degrees generally classify as cam morphology [3]. A recent study found that individuals with a severe cam-type deformity (alpha angle > 83 degrees) demonstrated an odds ratio of 10.88 (95% CI 5.21-22.69) for developing end-stage osteoarthritis [3]. Moreover, the risk of requiring THA with an alpha angle exceeding 83 degrees reached 23.3% [4].
Overlap between FAI and borderline dysplasia
Interestingly, radiographic FAI morphology rarely exists in isolation. Studies have found FAI present in 40-75% of patients with hip dysplasia [4]. This overlap creates a diagnostic challenge since borderline hip dysplasia is particularly common in young adults with hip pain, showing a reported prevalence of 37.6% in selected patient cohorts [4].
The spectrum of hip pathology ranges from unstable hips with shallow acetabuli to impinging hips with deep acetabuli [4]. A borderline hip (typically defined by a lateral center edge angle between 20-25 degrees) occupies the middle ground and may exhibit instability, impingement, or both [4]. This diagnostic complexity significantly impacts treatment decisions.
Recent evidence suggests that arthroscopic hip surgery with labral repair and capsular plication in patients with borderline dysplasia (LCEA > 20°) may yield appropriate short-term improvements [4]. Nevertheless, a prior ill-advised hip arthroscopy can negatively affect outcomes for these patients [4].
Patient Selection Criteria and Preoperative Risk Factors
Proper patient selection stands as the cornerstone of successful surgical intervention for FAI. When we select a total hip for these patients, we are very careful to select the bearing surface that gives them the longest survivorship, the prosthesis survivorship, and also minimize dislocation. Careful preoperative assessment through radiographic measurements and clinical factors helps identify patients who will benefit most from arthroscopic procedures while flagging those at risk for early conversion to THA.
Lateral center-edge angle (LCEA) thresholds for dysplasia
The lateral center-edge angle serves as a fundamental radiographic parameter for evaluating acetabular coverage of the femoral head. This measurement helps surgeons distinguish between normal hips, dysplastic hips, and those with pincer-type impingement. According to current literature, LCEA measurements fall into several distinct categories:
- <20°: Indicates acetabular dysplasia [5]
- 20-25°: Classified as borderline acetabular dysplasia (BDDH) [5]
- 25-40°: Considered normal acetabular coverage [5]
- 40°: Suggests pincer morphology of FAI [5]
Controversy exists regarding borderline dysplasia thresholds, with some studies defining it as an LCEA between 18-25° when measured from the bone edge on preoperative weight-bearing anteroposterior pelvic radiographs [6]. In fact, prior studies classified an LCEA <20° as developmental dysplasia of the hip (DDH) [6].
The measurement technique also matters significantly. The lateral acetabular rim method typically overestimates coverage by approximately 4° compared to the acetabular sourcil method since it includes non-weight-bearing bone that forms part of the labral base [5]. Most studies consider 40° as the upper limit of normal for LCEA and use the lateral edge of the sourcil as the reference point [7].
Tönnis angle and joint space narrowing
The Tönnis angle—measured as a line parallel to the horizontal plane of the pelvis and a tangential line extending from the medial edge to the lateral edge of the acetabular sourcil—provides another important radiographic parameter [6]. This measurement, alongside joint space assessment, helps predict outcomes after hip preservation procedures.
Joint space narrowing consistently emerges as a powerful predictor of failure following arthroscopic intervention. Research demonstrates a clear correlation between preoperative joint space and outcomes:
- 12% failure rate with slight or no preoperative joint space narrowing [8]
- 33% failure rate with mild to moderate preoperative joint space narrowing (<50% narrowing or >2mm joint space) [8]
- 82% failure rate with advanced preoperative joint space narrowing (>50% narrowing or ≤2mm joint space) [8]
Accordingly, the presence of Tönnis grade 1 osteoarthritis increases conversion risk to THA compared to grade 0 (42.9% vs 14.3%) [9]. Consequently, surgeons frequently exclude patients with advanced-level hip osteoarthritis (Tönnis Grade >1) from arthroscopic procedures [7].
Age and symptom duration as predictors of THA conversion
Age consistently appears as a significant risk factor for early conversion to THA. Patients who failed arthroscopic treatment were substantially older (41.0 ± 7.11 years) compared to those with successful outcomes (30.8 ± 8.39 years) [10]. Indeed, studies examining patients who underwent core decompression found that patients between 40-59 years had the highest rates of conversion to THA (61.1%, 138/226) [11].
Duration of preoperative symptoms also plays a crucial role in predicting outcomes. The failure cohort typically demonstrates a longer symptomatic period prior to surgical intervention (28.2 ± 11.4 months) compared to the successful treatment group (18.8 ± 7.41 months) [10].
Besides age and symptom duration, other variables associated with increased risk of conversion to THA include:
- Body mass index ≥25 kg/m² [9]
- Full-thickness acetabular chondral lesions, with significantly higher rates in failure cohorts (32% compared with 3%) [10]
- Need for microfracture procedure (hazard ratio 5.405, 95% CI: 1.876–15.384) [12]
- Higher preoperative and postoperative alpha angles [10]
A predictive model (THA-10 score) assigns points to various risk factors: 1 point for BMI ≥25 kg/m², 1 point for Tönnis grade 1, 2 points for age ≥47 years, and 3 points for high-grade defects of the acetabulum or femoral head [9]. Patients scoring ≥4 points were 13.2 times more likely to undergo THA conversion [9].
Surgical Outcomes and Long-Term Survivorship
Long-term data regarding surgical interventions for femoroacetabular impingement (FAI) reveals varying rates of success and failure across different techniques and patient populations. Understanding these outcomes helps surgeons make informed decisions about appropriate interventions. This raises conflict because you want to use a small femoral hand, so they have a thicker polyethylene, and hence the hip lasts long, but on the other hand, small femoral head puts them at a higher risk of dislocation.
The exciting trend here is the emergence of the Reverse Hip Replacement System (Reverse HRS). The Reverse HRS offers a unique option for these patients, because the wear of the reverse hip is very, very minimal based on the tribology data that we have, and then, of course, provides immense stability. So, this will be a real great option for this patient population.
Reverse Hip Replacement System
The Reverse Hip Replacement System (Reverse HRS) represents a significant advancement in hip replacement technology. This innovative Metal-on-Polyethylene reverse geometry hip prosthesis differs from conventional systems by positioning the ball within the acetabular cup instead of the femoral stem. Currently undergoing clinical investigation, the Reverse HRS has demonstrated promising results through extensive testing in over 100 pre-clinical experiments. This system aims to enhance stability during extended ranges of motion while reducing dislocation risks, particularly benefiting patients with complex hip conditions, such as dysplasia and FAI. THA instability and dislocation remains a significant possible complication and is more likely in patients with spinal fusion and certain surgical approaches. The Reverse HRS holds promise as it addresses this problem by allowing increased range of motion without impingement or dislocation.
The exceptional stability of the Reverse HRS derives from its unique component interaction. As the hip undergoes flexion-extension, abduction-adduction, and internal-external rotation, the femoral cup overlaps and articulates with the acetabular cup. This interlocking mechanism significantly reduces impingement and dislocation risk. Clinical testing has demonstrated that dislocation with the Reverse HRS requires both traction and laterally directed force in neutral position — a combination rarely occurring in normal movement patterns.

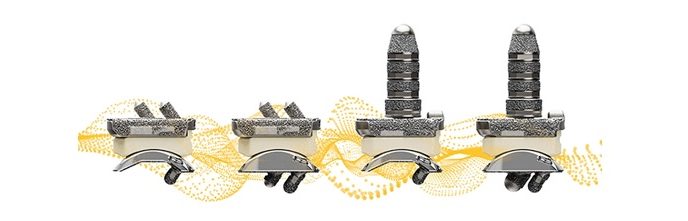
Figure 1: The current Reverse HRS Product Family includes Standard and High offset component devices.
Clinical Implications for Hip Arthroscopy in FAI Patients
Hip preservation procedures demand careful consideration of surgical technique and patient-specific factors. Appropriate intervention selection directly influences outcomes in FAI management.
Labral preservation vs debridement outcomes
Evidence increasingly supports labral preservation over debridement in hip arthroscopy. Studies show labral repair results in superior outcomes compared to debridement, with higher raw iHOT-12 scores at six months (58.9 vs 55.9) and 12 months (61.9 vs 57.4) postoperatively [10]. Correspondingly, a higher percentage of patients achieve substantial clinical benefit with labral repair (51.2%) versus debridement (43.9%) at 12-month follow-up [10]. The biomechanical rationale stems from the labrum’s crucial role in joint lubrication, cartilage nutrition, and load distribution [11].
Capsular plication in borderline dysplasia
For patients with borderline dysplasia (LCEA between 18° and 25°), capsular plication during arthroscopy has proven both safe and effective [12]. Ten-year survivorship data reveals 82.2% of these patients avoid conversion to THA [13]. Preoperative risk stratification remains essential, as patients older than 35 years demonstrate 2.25 times higher failure risk [32], while those ≥42 years face 7.1 times higher odds of THA conversion [14].
When to consider periacetabular osteotomy (PAO)
Periacetabular osteotomy becomes the preferred intervention for more severe dysplasia (LCEA <10-20°) [14]. Primary PAO indications include persistent pain, adequate ROM, and radiographic evidence of residual hip dysplasia [33]. Ideal candidates show joint space wider than 2mm and preoperative improvement in joint congruency on abduction radiographs [15]. Ultimately, PAO outcomes prove most predictable for hips with minimal preoperative osteoarthritis [16].
Conclusion
FAI presents a complex challenge in hip preservation surgery that demands thorough assessment and individualized treatment planning. Throughout this review, we examined how FAI significantly impacts total hip arthroplasty outcomes and identified crucial factors that influence long-term success. Radiographic parameters certainly play a vital role, with lateral center-edge angle, alpha angle, and joint space measurements serving as essential predictive tools.
Age consistently emerges as a powerful predictor of conversion to THA, with patients over 40 showing substantially higher failure rates after arthroscopic intervention. Additionally, symptom duration before surgery significantly affects outcomes, underscoring the importance of timely intervention. Full-thickness chondral lesions likewise correlate strongly with early failure, thus necessitating careful preoperative evaluation.
Surgical technique selection remains paramount for optimizing results. Labral preservation demonstrates superior outcomes compared to debridement, while capsular plication shows promise for patients with borderline dysplasia. Nevertheless, periacetabular osteotomy becomes necessary for more severe cases of acetabular dysplasia.
The overlap between FAI and borderline dysplasia creates diagnostic challenges yet offers opportunities for targeted interventions. Survivorship analyzes reveal encouraging long-term results for contemporary techniques, though revision rates vary considerably based on patient factors and surgical approach. And, emerging new prosthetic options, such as the Reverse HRS, can play a role in the improved management of these complex FAI patients.
Patient selection ultimately determines surgical success. The presence of advanced joint space narrowing, Tönnis grade >1 osteoarthritis, or full-thickness cartilage damage should prompt careful consideration before proceeding with arthroscopic intervention. Despite ongoing challenges, modern hip preservation techniques offer promising pathways for appropriately selected patients, potentially delaying or even preventing the need for total hip arthroplasty.
Orthopedic surgeons must therefore approach each FAI case individually, considering the complex interplay between morphological variants, patient characteristics, and surgical options. The field continues to evolve, with refined techniques and improved understanding of predictive factors steadily enhancing our ability to preserve hip function and improve quality of life for patients suffering from this challenging condition.
References
[1] – https://pubmed.ncbi.nlm.nih.gov/14646708/ Clin Orthop Relat Res. 2003 Dec:(417):112-20. doi: 10.1097/01.blo.0000096804.78689.c2.
[2] – https://www.ncbi.nlm.nih.gov/books/NBK547699/
[3] – https://radiologyassistant.nl/musculoskeletal/hip/femoroacetabular-impingement-syndrome
[4] – https://pmc.ncbi.nlm.nih.gov/articles/PMC5961333/
[5] – https://academic.oup.com/jhps/article/11/3/167/7596281
[6] – https://radiopaedia.org/articles/lateral-center-edge-angle-1?lang=us
[7] – https://pmc.ncbi.nlm.nih.gov/articles/PMC10549843/
[8] – https://journals.lww.com/md-journal/fulltext/2024/11220/lateral_center_edge_angle_in_femoroacetabular.57.aspx
[9] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3094626/
[10] – https://www.arthroscopyjournal.org/article/S0749-8063(24)00130-0/fulltext
[11] – https://boneandjoint.org.uk/Article/10.1302/2633-1462.34.BJO-2022-0003.R1
[12] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3470656/
[13] – https://www.sciencedirect.com/science/article/pii/S1048666620300069
[14] – https://pubmed.ncbi.nlm.nih.gov/37083686/
[15] – https://pubmed.ncbi.nlm.nih.gov/30419179/
[16] – https://pmc.ncbi.nlm.nih.gov/articles/PMC3492602/

Javad Parvizi, MD, The International Joint Center, a part of the Acıbadem Healthcare Group
Dr. Parvizi, a board-certified Orthopedic Surgeon in the USA & UK, is a true expert in his field. With extensive training in the United Kingdom, the United States, and Switzerland, he brings a wealth of knowledge and experience to his practice. For over 20 years, he served as the Director of Clinical Research at the prestigious Rothman Orthopedic Institute in Philadelphia, PA. Holding the esteemed James Edwards Professor Chair of Orthopedics at Thomas Jefferson University, Dr. Parvizi is a trusted authority in the management of complex hip and knee conditions, specializing in young patients with hip disorders. Renowned worldwide for his expertise in periprosthetic joint infection, joint preservation, and joint reconstruction, Dr. Parvizi is dedicated to providing the highest level of care to his patients.