An Improved Design with Special Benefits for Spinal Pelvic Disorders
July 6, 2026 / OrthoSpineNews / – The Reverse Hip Replacement trial at Tampa General Hospital (TGA) is part of a multicenter FDA-approved Investigational Device Exemption (IDE) study evaluating the Hip Innovation Technology (HIT) Reverse Hip Replacement System (Reverse HRS) for patients undergoing total hip arthroplasty.
“Tampa General is participating in this innovative trial through its orthopedic research and clinical innovation programs and in partnership with Tampa’s Florida Orthopedic Institute (FOI),” said Thomas Bernasek, MD. “The hospital’s involvement reflects its broader commitment to conducting investigational device trials and advancing orthopedic care through clinical research.” Dr. Bernasek is one of the lead investigators of this IDE study.
The Reverse Hip Replacement System (Reverse HRS) is considered advantageous for patients with spinopelvic disorders because these patients often have a higher risk of hip instability and dislocation after conventional total hip arthroplasty.
Overview
Total hip arthroplasty (THA) remains one of the most successful orthopedic procedures for restoring mobility and reducing pain in patients with degenerative hip disease. Despite advances in implant materials and surgical techniques, instability and postoperative dislocation continue to represent significant clinical challenges.
The Reverse HRS, developed by HIT, introduces a novel reverse-geometry design intended to improve joint stability and expand the functional range of motion. Following the FDA’s approval of this IDE, the system entered clinical evaluation to assess its safety and effectiveness in primary total hip arthroplasty.
Introduction
Conventional total hip replacement systems utilize a femoral head attached to the femoral stem that articulates within a polyethylene liner housed inside the acetabular component. While this configuration has demonstrated long-term success, implant instability remains a concern, particularly among patients with elevated dislocation risk.
To address these limitations, engineers and orthopedic innovators have explored alternative biomechanical configurations. One such innovation is the Reverse HRS, which reverses the traditional ball-and-socket arrangement while maintaining compatibility with established arthroplasty principles.
Reverse HRS Design Concept
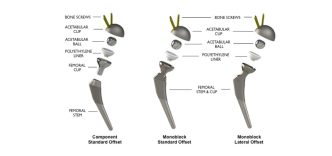
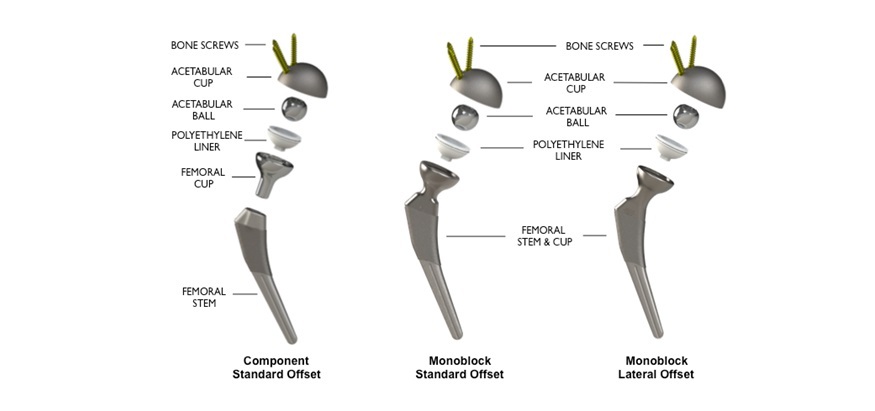
The Reverse HRS employs a reverse-geometry architecture in which the cobalt-chromium ball component is positioned within the acetabular cup rather than on the femoral stem. The polyethylene liner is attached to a femoral cup that interfaces with the femoral stem.
This configuration differs fundamentally from conventional THA designs by relocating the center of articulation and modifying joint mechanics. The primary design objectives include enhanced hip stability at extreme ranges of motion, reduced risk of prosthetic dislocation, greater flexibility in component positioning, and improved biomechanical performance during daily activities.
Reverse HRS – A Strong Legacy of Clinical Research
Clinical data on the Reverse HRS highlights excellent long-term implant fixation and notably low dislocation risks. The Reverse HRS has been extensively tested in over 100 standard and unique pre-clinical, bench level experiments assessing the product safety and clinical benefits anticipated by the reverse system design.
Thomas Turgeon, MD, Associate Professor, Max Rady College of Medicine, recently published 5-year follow-up from his radiostereometric analysis and clinical outcomes analysis of the Reverse HRS. This landmark five-year radiostereometric analysis (RSA) study has demonstrated exceptional implant-bone fixation stability and remarkably low wear rates for a revolutionary reverse total hip arthroplasty (RTHA) design, potentially transforming treatment outcomes for patients with severe hip osteoarthritis.
The study’s findings show femoral subsidence measurements consistently below 0.06mm and acetabular subsidence below 0.09mm at the five-year mark; significantly under published safety thresholds of 1.5mm and 1mm respectively. RSA analysis demonstrates excellent fixation with a predicted low risk of revision at ten years of this novel reverse total hip system. Clinical outcomes were consistent with safe and effective hip replacement prostheses.
“The bench level data compiled for the Reverse HRS exceeded all FDA requirements, setting the stage for the IDE study,” said Dr. Bernasek. “The clinical research performed in Canada demonstrated excellent prosthesis to bone interface stability as evidenced by RSA data. We are excited to be enrolling patients in this IDE clinical trial.”
The Spinopelvic Challenge
Published data reports that traditional THA systems are not as effective for patients with previous spinal fusion. This patient population may experience increased risk of dislocation due to alteration of the spinal pelvic mechanics. These biomechanical alterations are not adequately addressed by currently available conventional or dual mobility hip arthroplasty systems.
Also, data shows that compared to patients without lumbar fusion, patients with lumbar fusion demonstrated an 80% increase in dislocation at six months, 71% at one year and 60% at two years. There was also a 48% increased risk of any failure leading to revision hip surgery in patients with lumbar fusion at six months, 41% at one year, and 47% of two years.
The hip and spine function as a coordinated mechanical system. When a person sits, stands, bends, or walks, the pelvis rotates and changes the orientation of the hip socket.
In patients with conditions such as degenerative lumbar spine disease, prior lumbar spinal fusion, fixed sagittal imbalance, spinal stiffness, and adult spinal deformity, the pelvis may not rotate normally during movement.
This altered spinopelvic motion can change the functional position of the acetabular component after hip replacement, increasing the risk of impingement, edge loading, instability, and prosthetic dislocation.
How Reverse HRS May Help
The Reverse HRS uses a reverse-geometry articulation in which the ball component is located on the acetabular side. The polyethylene-bearing component is attached to the femoral side. This design is intended to provide increased stability.
“The geometry may increase resistance to dislocation during activities that place the hip at extreme positions,” said John M. Small, MD, Orthopedic Surgeon, Spine Expert, Florida Orthopedic Institute. “For patients whose pelvis cannot adapt normally during sitting or standing, additional intrinsic stability can be particularly valuable.”
The Reverse HRS design also delivers greater jump distance. “Jump distance” refers to how far the femoral component must travel before dislocation occurs. A larger effective jump distance generally improves implant stability.
Because spinopelvic disorders can alter the functional orientation of the hip socket throughout daily activities, implants that tolerate a wider range of component positions may perform better. The Reverse HRS was designed with this concept in mind. By modifying the articulation geometry, the system may allow greater motion before components impinge on each other, reducing one pathway leading to dislocation.
Why This Population Is Important
“Patients with spinal pathology are increasingly recognized as a high-risk group in hip arthroplasty,” explained Dr. Small. “Many orthopedic surgeons now routinely evaluate spinopelvic alignment before surgery because abnormal spine-pelvis mechanics can significantly affect hip replacement outcomes.”
The Reverse HRS is being investigated partly because it addresses the biomechanical challenges faced by these patients. Also of important note, The FDA has approved the Reverse HRS for Compassionate Use in patients with stiff spine or spinal fusion.
Clinical Study Objectives
The IDE study focuses on two primary endpoints – safety assessment and effectiveness assessment. The safety evaluation includes device-related adverse events, postoperative complications, revision surgery rates, and patient quality-of-life measurements.
Clinical effectiveness is measured through functional outcome scores, radiographic analysis, implant survivorship, patient-reported outcome measures, and assessment of postoperative stability and range of motion.
The study aims to determine whether the reverse-geometry design can achieve outcomes that are comparable or superior to conventional hip replacement systems.
Future Outlook
The Reverse Hip Replacement System represents one of the most innovative developments in contemporary hip arthroplasty design. If the ongoing IDE studies demonstrate improved stability, lower dislocation rates, and durable implant performance, reverse-geometry hip replacement could become a standard option for THA.
Conclusion
The Reverse HRS introduces a novel reverse-geometry concept intended to address one of the most persistent challenges in total hip arthroplasty: postoperative instability. Supported by an FDA-approved IDE study, the device is undergoing rigorous clinical evaluation to determine its safety and effectiveness.
The Reverse HRS represents an excellent option for patients with spinopelvic disorders because its reverse-geometry design may provide greater stability, reduce dislocation risk, and better accommodate abnormal spine-pelvis mechanics than conventional hip replacement systems.
Thomas L. Bernasek, MD

Thomas L. Bernasek, MD, is fellowship-trained in adult reconstruction. Prior to becoming a founding member of Florida Orthopaedic Institute, Dr. Bernasek received his medical training at the Creighton University College of Medicine in Omaha, Nebraska, and completed his Orthopedic Residency training at the University of New Mexico. After residency, Dr. Bernasek completed a fellowship in joint replacement and adult reconstruction at the Mayo Clinic in Rochester, Minnesota.
He is known nationally and internationally as an expert in joint replacement with vast experience in total hip and knee replacement. His articles have been published in numerous professional journals, and he has presented research papers and lectured at medical conferences on the national and international level for over a decade. He maintains active involvement in numerous orthopedic research and development projects and has served as a professor in orthopaedic surgery at the University of South Florida College of Medicine. Dr. Bernasek served as the President of Hillsborough County Medical Association.
John M. Small, MD

Dr. John M. Small is a board-certified orthopedic surgeon specializing in spine surgery. He has been with the Florida Orthopaedic Institute since 1996. Dr. Small completed his medical education at the University of Nebraska Medical Center, where he also earned a Doctor of Pharmacy degree.
He completed his orthopedic surgery residency at the University of Texas Southwestern Medical Center in Dallas and a spine surgery fellowship at the Kerlan-Jobe Orthopaedic Clinic in Los Angeles. Dr. Small has comprehensive training in cervical, thoracic, and lumbar spine care, with a special interest in sports-related injuries.
He is an Associate Assistant Professor at the University of South Florida Department of Orthopaedics and serves as the Residency Site Director at the University Community Hospital. Dr. Small has been named a Best Doctor of America every year since 2005. His personal interests include running, biking, and participating in triathlons.